Chronic Care Management Services
Circle Care's AI-powered CCM platform identifies every eligible patient, coordinates every care plan, and keeps your team CMS-compliant — improving chronic care outcomes and unlocking sustainable practice revenue from day one.
CCM Compliance at a Glance
- Real-time identification of eligible Medicare patients
- Digital patient consent captured and documented
- CMS-compliant care plan created and assigned
- 20-minute monthly threshold tracked automatically
- Monthly interactions logged with time-stamped records
- CPT 99490, 99439, 99487 or 99489 auto-applied
- Full audit trail for every CCM episode
What Is Chronic Care Management?
Chronic Care Management (CCM) is a structured, CMS-defined care program that provides continuous, coordinated support to Medicare patients living with two or more chronic conditions. Designed to close the gap between office visits, CCM covers a minimum of 20 minutes of non-face-to-face clinical care per calendar month — including care plan management, medication oversight, and coordination across providers and specialists.
Who Qualifies for CCM?
- Medicare Part B beneficiary (including Medicare Advantage)
- Two or more chronic conditions expected to last 12+ months or until death
- Conditions place the patient at significant risk of acute exacerbation, functional decline, or death
- Patient provides informed consent (written or verbal), documented in the medical record
- Not receiving CCM from another provider in the same calendar month
Qualifying conditions include:Diabetes · Hypertension · Heart Disease · COPD · Depression · Chronic Kidney Disease · Alzheimer's Disease · and many more
CCM vs. Standard Care Between Visits
| Area | Traditional Care | CCM with Circle Care |
|---|---|---|
| Patient contact | Patient-initiated | Proactive monthly outreach — automated |
| Care plan | Generic or paper-based | Condition-specific, digital, CMS-compliant |
| Medication review | At appointment only | Ongoing reconciliation and adherence tracking |
| Care coordination | Ad hoc | Structured, documented, trackable |
| Billing | Standard E&M codes | CPT 99490 / 99439 / 99487 / 99489 auto-applied |
| Readmission risk | Unmanaged | Actively reduced with real-time monitoring |
| Compliance tracking | Manual or none | AI-powered, full audit trail |
Chronic Care Management Under Medicare — What Providers Need to Know
CMS defines CCM as a set of coordinated services delivered to Medicare beneficiaries with two or more chronic conditions — designed to improve outcomes, reduce avoidable hospitalisations, and support proactive disease management between office visits. Four CPT codes govern reimbursement based on service complexity and time spent per calendar month.
Circle Care's platform is built around these CMS requirements. Every consent, care plan, interaction, and time entry is tracked, time-stamped, and audit-ready before a claim is ever submitted.
CMS Requirements & Patient Consent
Medicare patients must have two or more qualifying chronic conditions and provide documented consent before CCM services begin. Consent must be renewed annually. Circle Care's enrollment workflow captures consent digitally, timestamped, and stored in the patient's record — so your team is protected, and your program is billable from day one.
Non-Face-to-Face Care Coordination
At least 20 minutes of clinical staff time must be spent per calendar month on non-face-to-face CCM activities — including phone calls, care plan updates, medication management, referral coordination, and patient education. Circle Care auto-tracks time across every patient interaction, so the monthly threshold is never missed.
Medicare Coverage & Co-Pay Considerations
Medicare Part B covers CCM services, with patients typically responsible for a 20% co-pay. CCM can be billed alongside an Annual Wellness Visit (AWV) in the same month, making the AWV a natural CCM enrollment trigger. Only one provider may bill CCM for a given patient per calendar month. Circle Care flags code conflicts automatically before any claim is submitted.
Everything You Need for CCM Success
Circle Care's CCM software handles the entire chronic care workflow — real-time patient identification, care plan creation, monthly care coordination, time tracking, and billing — so your team focuses on patients, not paperwork. No upfront investment. No new staff required.
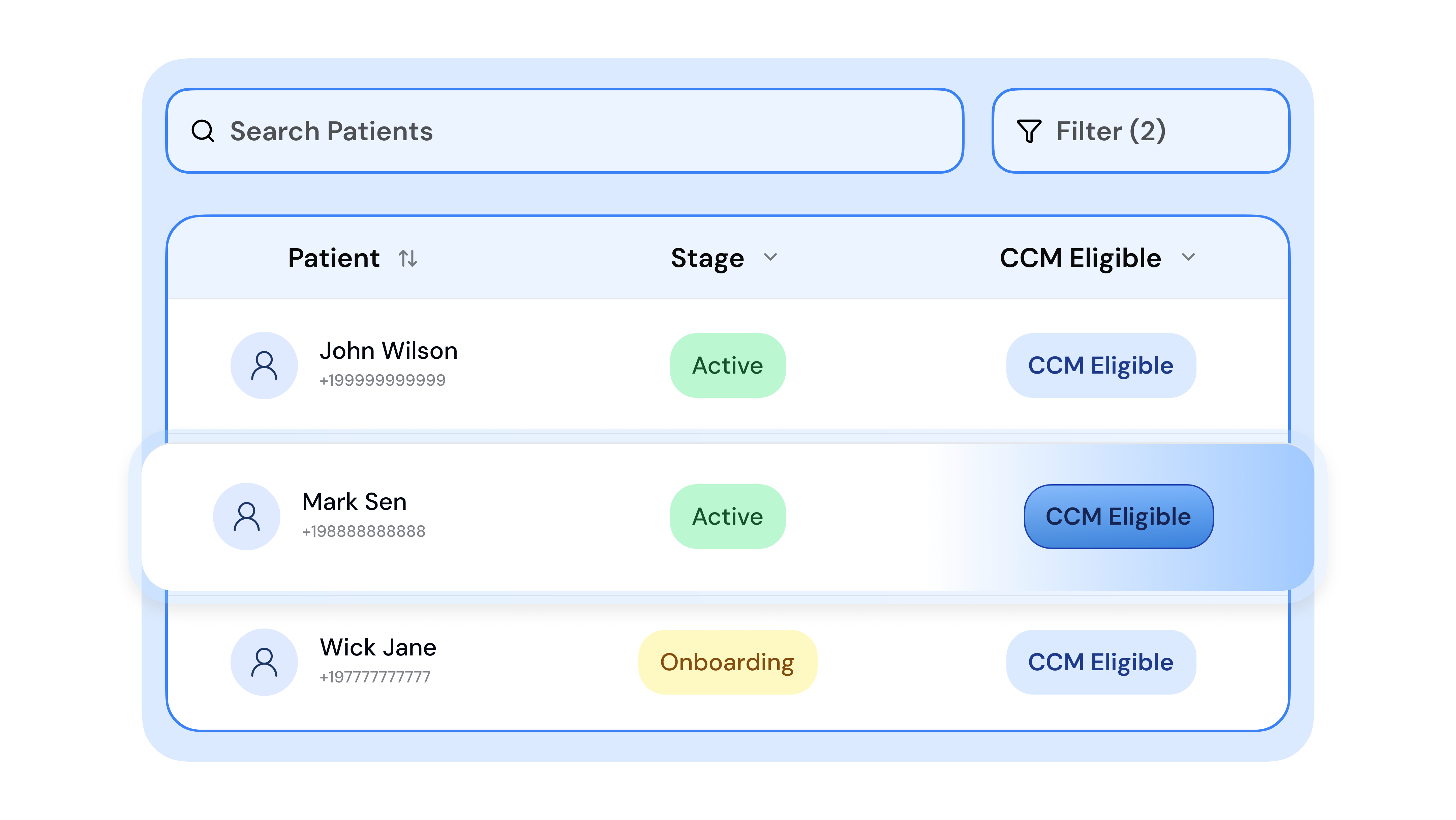
Spot Eligible Patients Instantly
Get real-time alerts when patients qualify for CCM. Circle Care's AI-powered identification engine integrates with your EHR and Annual Wellness Visit data to surface eligible Medicare patients automatically — so enrollment starts the moment a patient qualifies, not weeks later. No manual chart reviews. No missed opportunities.
Stay Audit-Ready and Compliant
Automated checks and reminders keep your team aligned with CMS documentation standards at every step. Consent records are timestamped and stored. Care plans are version-controlled. Every interaction is logged with user attribution. If CMS comes looking, Circle Care gives you everything you need to respond in seconds.
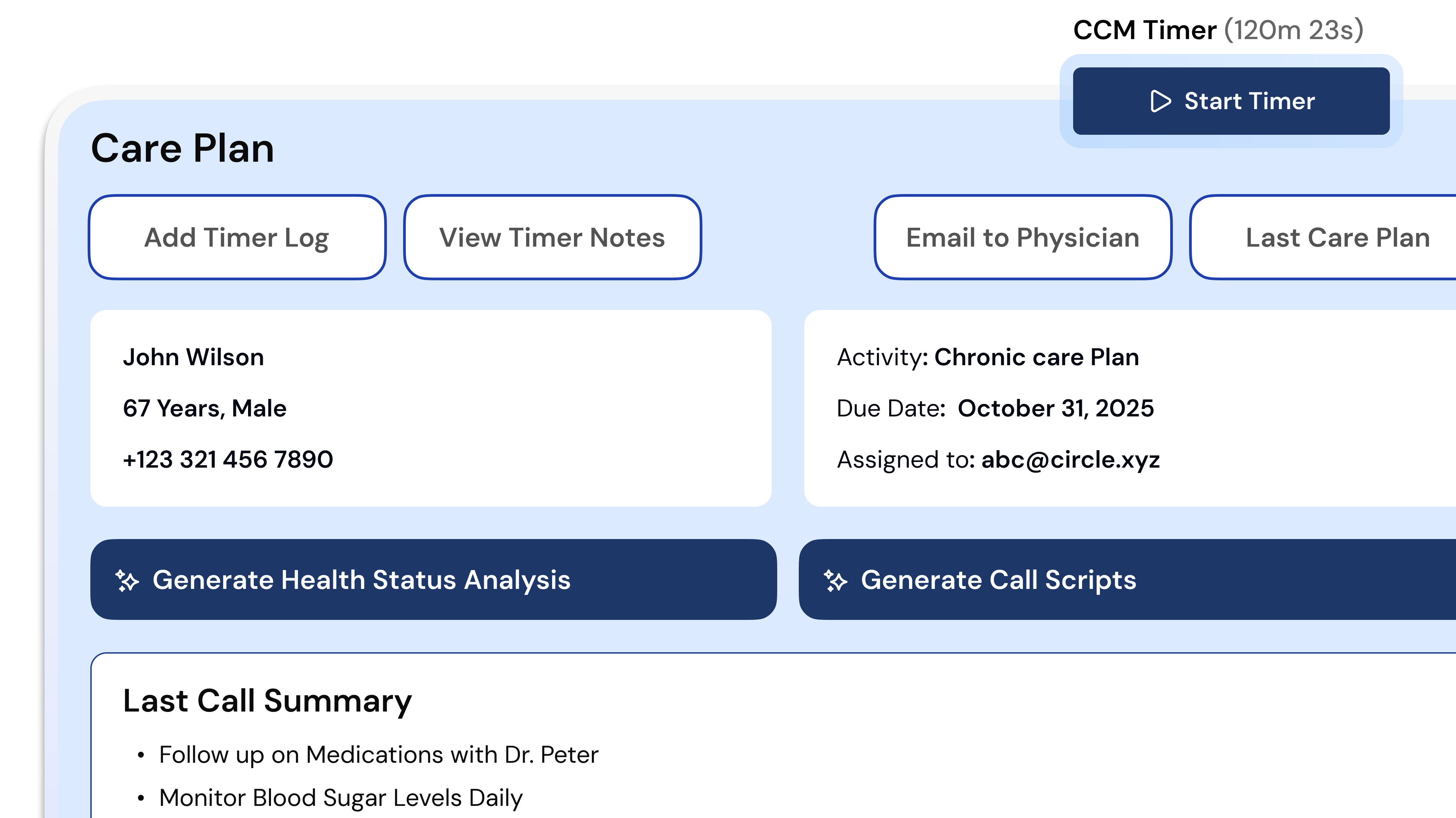
Build Personalised Care Plans in Minutes
Creating a CMS-compliant care plan for every enrolled patient used to mean hours of documentation. Circle Care replaces that burden with condition-specific, editable templates pre-loaded with CMS-required elements and organised by chronic condition. Practitioners review, confirm, and customise rather than build from scratch.
Turn Data into Action with AI-Driven Intelligence
Uncover patterns, risks, and care gaps in real time. Circle Care's clinically trained AI reviews patient history, flags deteriorating trends, and delivers actionable insights — so your care team can intervene earlier, personalise outreach, and drive measurably better outcomes for your highest-risk patients.

Turn Patient Support into Sustainable Revenue
Circle Care simplifies Medicare CCM compliance and billing, ensuring your team is reimbursed for every qualified 20-minute monthly interaction without adding extra administrative work. Time tracking begins automatically the moment a care manager opens a patient record, and the platform alerts your team when the billing threshold is met.
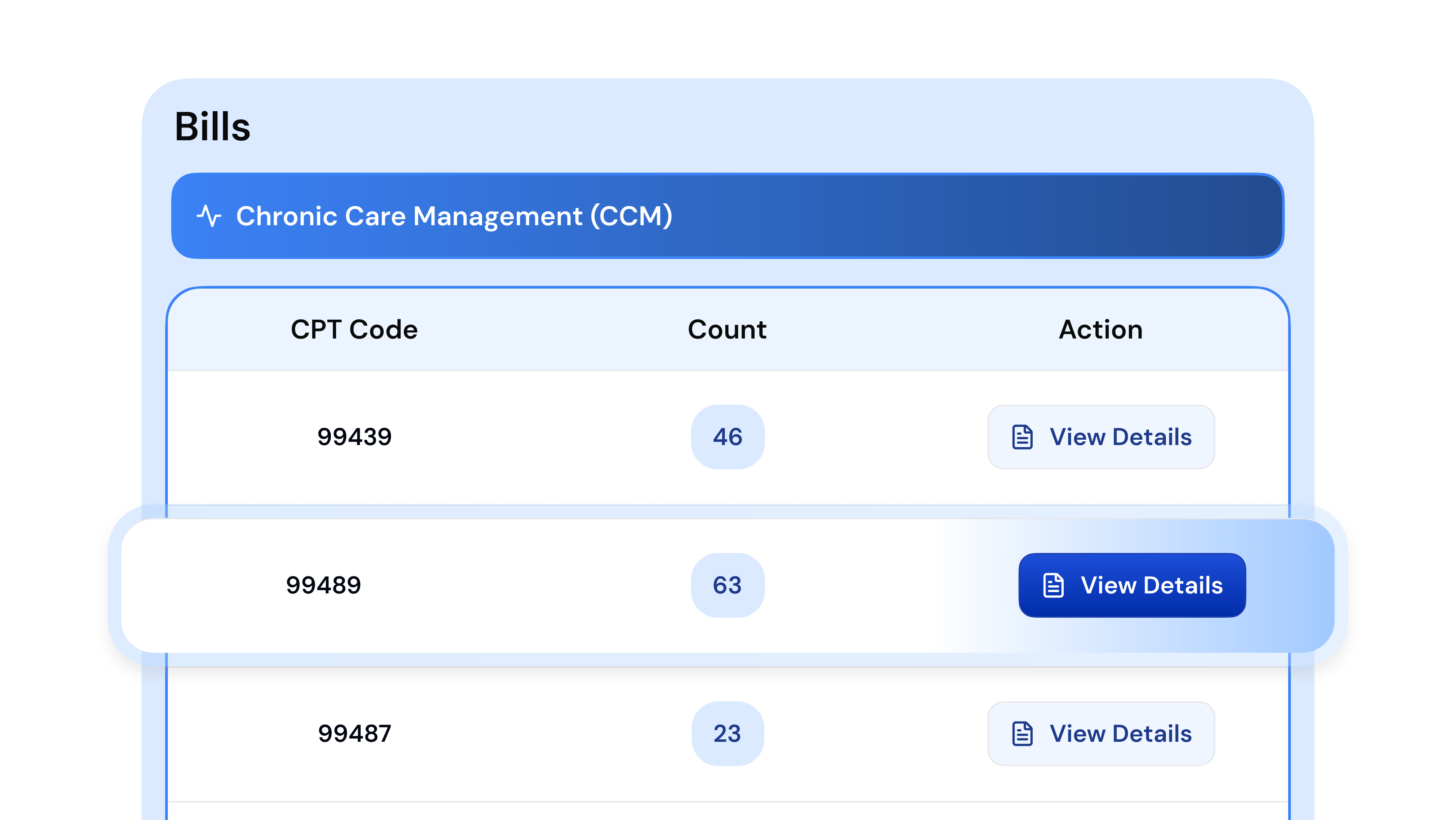
Simplify Your CCM Revenue Cycle
Track every patient interaction effortlessly and consolidate them into one ready-to-bill report. Circle Care maps all activity to the correct CPT code, runs a billing readiness check for each patient, and exports a clean, submission-ready report to your billing team or clearinghouse. Review, approve, and submit — it's that seamless.
Billing & Codes
Auto-capture time & notes to bill accurately for CPT 99490, 99439, 99487 & 99489
EHR Integration
FHIR/HL7-compatible. Connects with major EHRs to eliminate double entry
Security & Compliance
HIPAA, SOC 2 Type II, ISO 27001. Enterprise-grade encryption and role-based access
The CCM Process with Circle Care: Step by Step
Circle Care structures CCM delivery across four CMS-aligned phases. Every milestone is tracked, documented, and flagged within the platform — so no episode falls through the cracks, and no revenue is left on the table.
Identify & Enroll Eligible Patients
- AI-powered engine surfaces eligible Medicare patients from your EHR in real time
- Patients with 2+ qualifying chronic conditions are flagged and prioritised automatically
- Digital consent workflow captures and timestamps patient agreement
- Enrolled patients are assigned to a licensed care manager immediately
Build & Assign Care Plans
- Condition-specific care plan templates pre-loaded with CMS-required elements
- Practitioner reviews, customises, and finalises the plan within Circle Care
- Care plan shared across the care team and stored in the patient record
- Annual review reminders are generated automatically
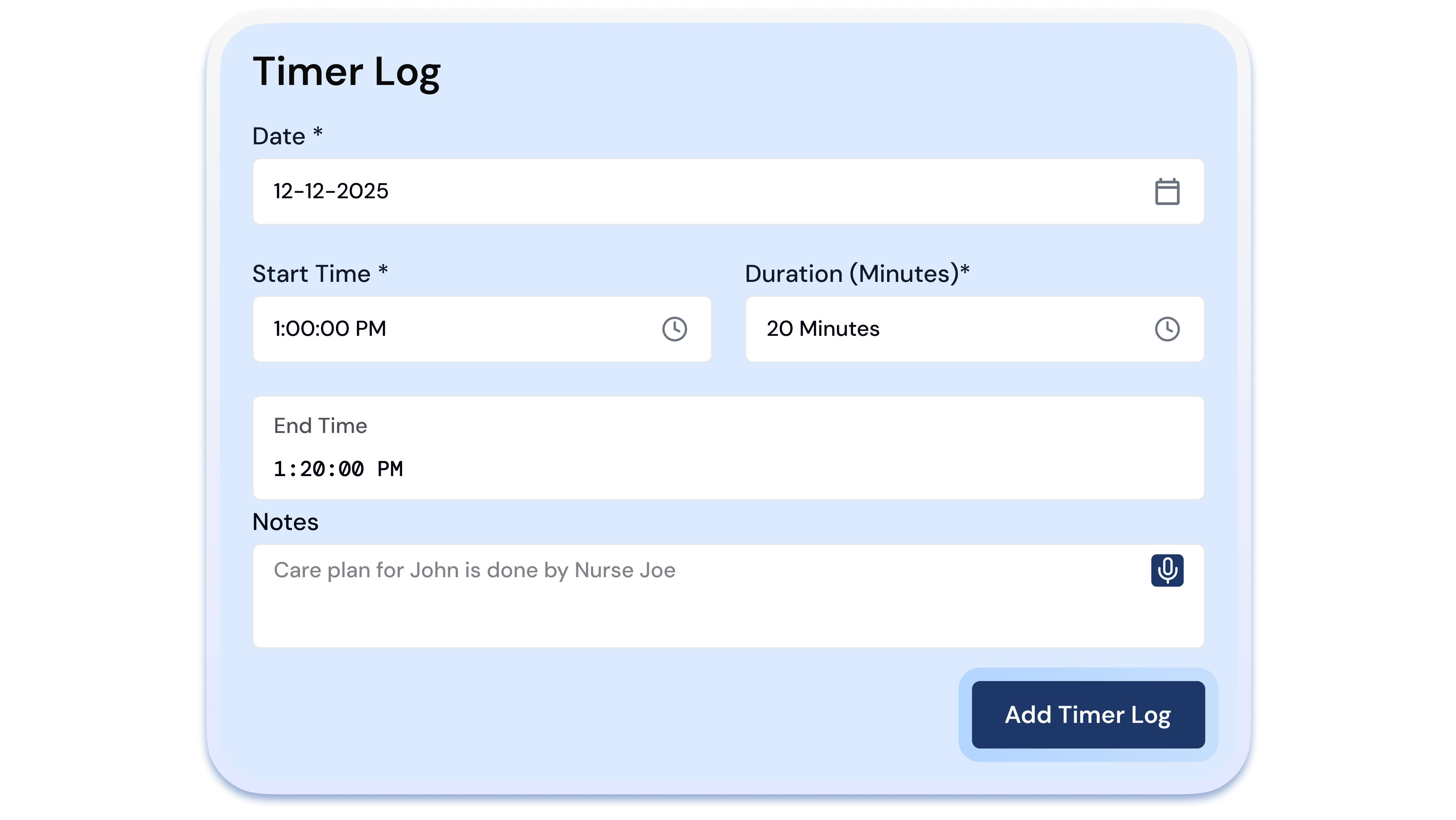
Log Monthly Interactions & Track Time
- Time tracking begins automatically when a care manager opens a patient record
- All calls, messages, medication reviews, and referrals are logged with timestamps
- The live dashboard shows time logged per patient against the 20-minute threshold
- Care managers are alerted when the monthly minimum is met and when follow-up is due
Generate Compliant Billing Reports
- All interactions consolidated into a single, submission-ready monthly billing report
- CPT code auto-assigned based on time logged and service complexity
- Billing readiness check flags incomplete documentation or code conflicts before submission
- Report exported directly to your billing team or clearinghouse for fast reimbursement
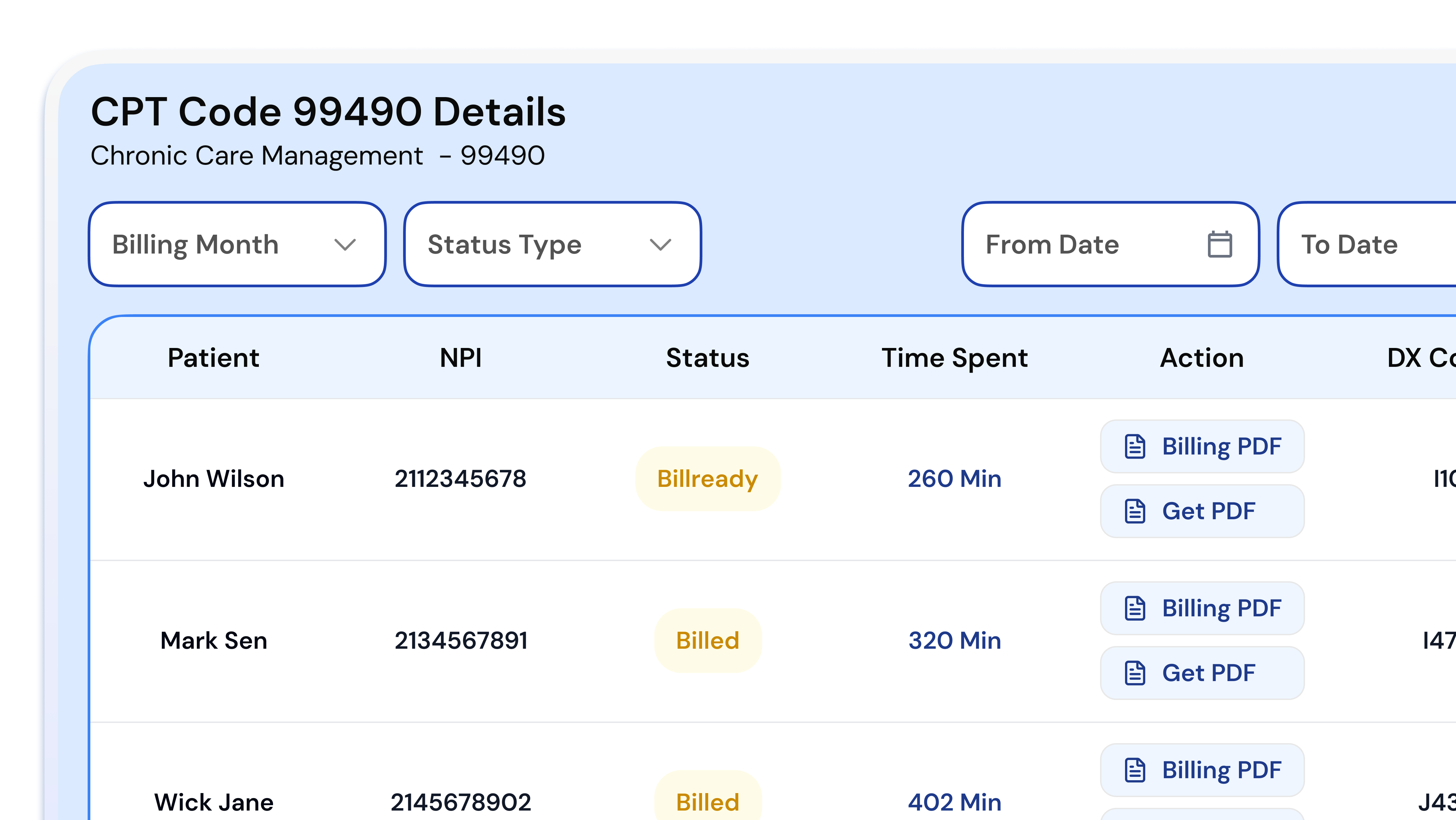
Chronic Care Management Billing & CPT Codes
Circle Care automatically applies the correct CCM CPT code — 99490, 99439, 99487, or 99489 — based on documented time, service complexity, and monthly activity. No manual code selection. No missed reimbursement.
- Service
- Standard CCM — first 20 minutes
- Time required
- At least 20 minutes/month of non-face-to-face care coordination
- Who bills it
- Clinical staff under physician supervision
- Average Medicare payment
- ~$64
- Who qualifies
- Medicare patients with 2+ chronic conditions
- Circle Care
- Auto-assigns code when 20-minute threshold is documented
- Service
- Standard CCM — each additional 20 minutes
- Time required
- Each additional 20-minute increment beyond CPT 99490
- Billed with
- CPT 99490
- Average Medicare payment
- ~$47
- Who qualifies
- Same patient, same month — additional time documented
- Circle Care
- Auto-adds units as time thresholds are met
- Service
- Complex CCM — first 60 minutes
- Time required
- At least 60 minutes/month
- Complexity required
- Moderate-to-high complexity MDM; physician or NPP involvement
- Average Medicare payment
- ~$92
- Who qualifies
- Patients with complex, multi-condition management needs
- Circle Care
- Complexity pulled from care plan documentation for accurate auto-assignment
- Service
- Complex CCM — each additional 30 minutes
- Time required
- Each additional 30-minute block beyond CPT 99487
- Billed with
- CPT 99487
- Average Medicare payment
- ~$45
- Who qualifies
- Same patient, same month, additional complex care time documented
- Circle Care
- Auto-assigns additional units based on logged time
Billing Best Practices
CCM claims are submitted monthly, with the service period covering the calendar month. Only one provider may bill CCM for a given patient per month, and CCM cannot be billed in the same month as TCM or PCM from the same provider. Circle Care's billing prep module runs a readiness check before any claim goes out, flagging incomplete documentation, unmet time thresholds, or code conflicts automatically.
Common Billing Errors Circle Care Prevents
Chronic Care Management Template — What a Compliant Care Plan Includes
Complete, accurate documentation is the foundation of a defensible CCM claim. Circle Care's built-in care plan templates pre-populate required fields from your connected EHR — reducing manual entry, minimising errors, and ensuring every enrolled patient is audit-ready from day one.
Required Documentation Checklist
- Problem list: All active chronic conditions documented
- Treatment goals: Measurable, condition-specific outcomes defined
- Medication list & allergy record: Current medications, dosages, and known allergies
- Symptom & self-management plan: Patient-facing guidance for daily management
- Care team contacts: Responsible provider and all coordinating clinicians identified
- Referrals & specialist coordination: Outgoing and incoming referrals tracked
- Follow-up schedule: Appointments, check-ins, and review dates logged
- Patient consent record: Date, method, and renewal status documented
Documentation Example Breakdown
“Verbal consent obtained 04/15/2025 at 9:30 AM by RN. Patient informed of CCM program, co-pay responsibilities, and right to opt out at any time. Consent logged and timestamped in Circle Care platform.”
“Active chronic conditions: Type 2 Diabetes (E11.9), Hypertension (I10), Stage 3 CKD (N18.3). Goals: HbA1c < 7.5%, BP < 130/80, eGFR stable over 90 days. Reviewed and updated 04/15/2025.”
“Phone contact 05/02/2025 at 2:15 PM by Care Manager. Patient reported medication side effects; physician notified, prescription adjusted. Time logged: 24 minutes. CPT 99490 threshold met. Logged in Circle Care platform.”
Chronic Conditions We Support
Circle Care's CCM program is built to support the full spectrum of conditions that place Medicare patients at the greatest risk. Each condition has dedicated care plan templates, evidence-based intervention checklists, and condition-specific monitoring protocols built directly into the platform.
Diabetes
Diabetes affects more than 37 million Americans and is one of the most common qualifying conditions for CCM. Circle Care's diabetes care plan templates cover blood glucose monitoring, medication adherence, dietary guidance, HbA1c tracking, and specialist coordination with endocrinologists and ophthalmologists.
Learn MoreHeart Disease & Hypertension
Cardiovascular disease remains the leading cause of death in the United States. Our CCM templates for heart disease and hypertension address medication management, blood pressure monitoring, weight tracking, lifestyle modification, and cardiology coordination — including post-discharge follow-up protocols.
Learn MoreCOPD & Respiratory Conditions
Patients with chronic obstructive pulmonary disease and other respiratory conditions require close monitoring to prevent exacerbations and emergency hospitalisations. Circle Care supports spirometry tracking, inhaler adherence, oxygen management, and pulmonologist coordination within the CCM framework.
Learn MoreDepression & Behavioral Health
Behavioral health conditions are among the most underserved in traditional care management. Circle Care integrates PHQ-9 tracking, depression screening, medication management, and warm handoffs to behavioral health providers — ensuring the whole patient is supported, not just their physical conditions.
Learn MoreChronic Kidney Disease
CKD progression is highly manageable when patients receive consistent monitoring and education. Our CKD templates include eGFR and creatinine tracking, dietary guidance, medication reconciliation, and nephrologist coordination — all documented within the CCM compliance framework.
Learn MorePair CCM with Other Value-Based Care Programs
CCM is one of six CMS care programs on Circle Care. Combine it with RPM, TCM, or BHI to build a complete, revenue-generating care ecosystem — all on one platform, one team.
Remote Patient Monitoring
Real-time vitals tracking to prevent complications and reduce hospital readmissions between appointments.
Learn MoreTransitional Care Management
Coordinated post-discharge support to reduce readmissions during the critical 30-day transition window.
Learn MoreBehavioral Health Integration
Integrate behavioral health into everyday primary care to address the whole patient, not just the condition.
Learn MorePrincipal Care Management
Focused management for patients with a single, high-risk chronic condition requiring intensive coordination.
Learn MoreAdvanced Primary Care Management
Population-based care management for practices delivering advanced, comprehensive primary care.
Learn MoreCare Management Services
Our team of licensed RNs and medical assistants works as an extension of your practice. No new hires needed.
Learn More“Circle Care has transformed the way we deliver care — helping us spot gaps early, stay connected with patients between visits, and act faster when it matters most. Their team feels like an extension of ours, combining smart technology with real, human support.”
Chronic Care Management — Questions Answered
CCM is a structured CMS care program providing continuous, coordinated support to Medicare patients with two or more chronic conditions. It includes proactive monthly outreach, care plan management, medication reconciliation, and specialist coordination, all designed to improve disease management and prevent avoidable hospitalisations. Circle Care automates the entire process.
Patients must be Medicare Part B beneficiaries with two or more chronic conditions expected to last at least 12 months or until death, where those conditions place them at significant risk of acute exacerbation or functional decline. Informed consent must be documented before services begin. Circle Care's platform identifies and flags eligible patients automatically from your EHR.
CMS requires: (1) two or more qualifying chronic conditions; (2) a comprehensive, documented care plan; (3) a minimum of 20 minutes of non-face-to-face clinical staff time per calendar month; and (4) documented patient consent. Circle Care tracks every requirement in real time and prompts your team before any deadline is missed.
CPT 99490 covers standard CCM for the first 20 minutes of clinical staff time per month (avg. payment ~$64). CPT 99487 covers complex CCM requiring moderate-to-high complexity medical decision-making and at least 60 minutes of clinical staff time per month (avg. payment ~$92). Circle Care auto-assigns the correct code based on documented time and service complexity.
Revenue depends on the number of enrolled patients and the CPT codes billed. A practice with 200 eligible Medicare patients and an 85% enrollment rate can generate an estimated $18,700 or more in monthly reimbursement. Use Circle Care's revenue calculator to estimate your potential.
Yes. CMS allows CCM and the Annual Wellness Visit (AWV) to be billed in the same calendar month, provided the CCM care plan is initiated or updated during the AWV encounter. This makes the AWV a natural and highly effective CCM enrollment trigger. Circle Care flags this linkage during the enrollment workflow.
Yes. CCM and Remote Patient Monitoring (RPM) can be billed concurrently for the same patient, provided all time and documentation requirements for both programs are independently met. Circle Care supports both programs within a single platform and flags any code conflicts before submission.
A CMS-compliant CCM care plan must include: the patient's problem list, measurable treatment goals, current medications and allergies, symptom management guidance, care team contacts, referral and specialist coordination, a follow-up schedule, and documented patient consent. Circle Care's templates pre-populate all required fields from your connected EHR.
Most practices are live and billing within two weeks of onboarding. Circle Care handles EHR integration, patient identification, care manager setup, and compliance configuration so your team can focus on patient care from day one.
Yes. Circle Care is HIPAA compliant, SOC 2 Type II certified, and ISO 27001 certified. All patient data is encrypted at rest and in transit, with enterprise-grade role-based access controls and full audit logging on every interaction.
Latest Insights on Chronic Care Management
Operationalizing CCM Without Hiring New Staff in Skilled Nursing Facilities
SNFs can launch CCM programs without new staff. Learn eligibility, billing, staff roles, and how to build a sustainable care management program.
CPT Code 99490 for Billing Chronic Care Management
A practical breakdown of CPT 99490 — who qualifies, what documentation is required, and how to avoid the most common CCM billing errors.
What Is Chronic Care Management & How It Works
A complete guide to CCM — CMS requirements, eligible conditions, care plan essentials, and how Circle Care makes compliance effortless.
Ready to Start Your Chronic Care Management Program?
Let's design a CCM program that keeps your patients healthier between visits and grows sustainable practice revenue — with zero upfront cost and no new staff needed.