Principal Care Management Services
Not every patient needs CCM. Some need something more targeted. Circle Care's AI-powered PCM platform delivers intensive, condition-focused care for patients with one high-risk chronic condition while unlocking a separate, fully billable Medicare revenue stream for your practice.
PCM Compliance at a Glance
- Real-time identification of high-risk single-condition Medicare patients
- Digital patient consent captured and documented
- Condition-specific electronic care plan created and assigned
- 30-minute monthly threshold tracked automatically
- Monthly interactions logged with time-stamped records
- CPT 99424, 99425, 99426, or 99427 auto-applied
- Full audit trail for every PCM episode
What Is Principal Care Management?
Principal Care Management (PCM) is a Medicare-reimbursed care model focused on a single, serious chronic condition that requires complex, ongoing management for a period of three or more months. Introduced by CMS effective January 1, 2023, PCM fills a critical gap in the care management landscape for patients who have one dominant condition severe enough to demand its own dedicated coordination program.
PCM meaning in practice: it's intensive, not general. Unlike CCM, which covers patients with two or more chronic conditions, PCM is specifically designed to provide deep, condition-focused care coordination for the highest-risk patients in your panel. Circle Care makes that entire process automatic — from patient identification and consent through monthly interactions and billing submission.
Who Qualifies for PCM?
- Medicare beneficiary (Part B) with one serious, complex chronic condition
- Condition expected to last at least 3 months with risk of acute exacerbation, death, or functional decline
- Management unusually complex due to severity, comorbidities, or treatment burden
- Written informed consent obtained and documented before services began
- Services overseen by a physician or qualified non-physician practitioner (NPP)
- Only one provider per patient per month may bill PCM
Common qualifying conditions include:
PCM vs. CCM — Side by Side
| Feature | PCM | CCM |
|---|---|---|
| Conditions covered | 1 single high-risk/complex condition | 2+ chronic conditions |
| Condition severity | High-risk, complex, or comorbid | Any qualifying chronic condition |
| Monthly time minimum | 30 min (physician or clinical staff) | 20 min (clinical staff) |
| Who can bill | Physician, NPP, or supervised clinical staff | Clinical staff under general supervision |
| Care plan required | Yes — condition-specific | Yes — comprehensive, multi-condition |
| Base CPT code | 99424 (physician) / 99426 (staff) | 99490 |
| Avg. base reimbursement | ~$97 (physician) / ~$74 (staff) | ~$64 |
| One provider per patient | Yes | Yes |
| Effective date | January 1, 2023 | January 1, 2015 |
| Concurrent with RPM | Yes | Yes |
| Concurrent with CCM | No — cannot bill both same month | No — cannot bill both same month |
Principal Care Management Guidelines — CMS Rules & Requirements
CMS introduced PCM codes in 2023 to fill a gap in the care management landscape for patients who didn't qualify for CCM but still required intensive coordination for one complex condition. Five PCM codes became effective January 1, 2023, under the final 2023 Physician Fee Schedule. Understanding the rules is essential before billing.
Circle Care's platform is built around these CMS requirements. Every consent, care plan, interaction, and time entry is tracked, time-stamped, and audit-ready before a claim is ever submitted.
CMS Requirements & Patient Consent
Before billing any PCM code, written or verbal consent must be documented in the medical record — covering the scope of PCM services and applicable cost-sharing. The patient must be informed that only one provider may bill PCM per calendar month and that they may opt out at any time. Circle Care's digital enrollment workflow captures, timestamps, and stores consent automatically so your program is billable and protected from day one.
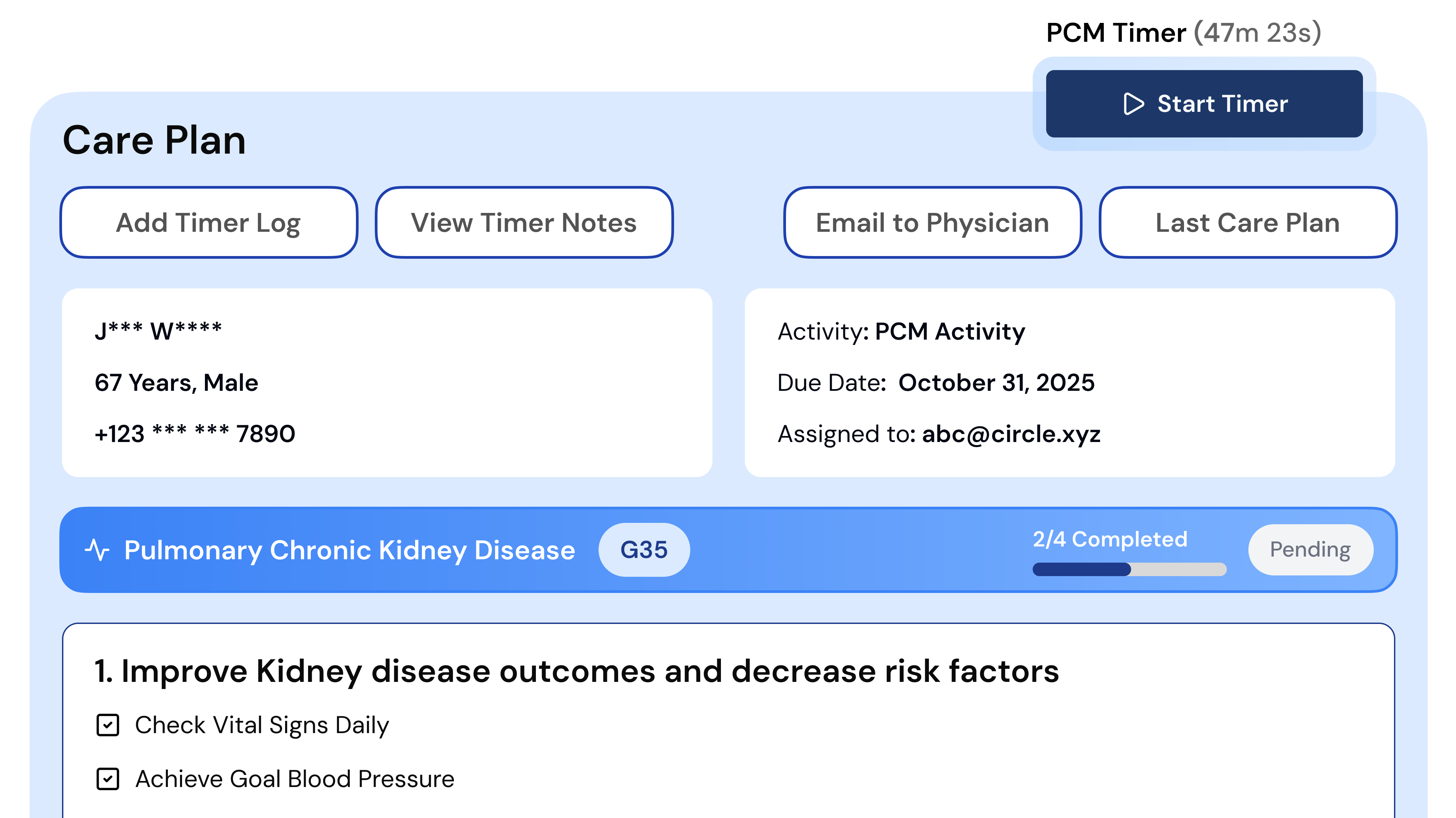
Condition-Specific Care Plan & Monthly Interactions
A comprehensive electronic care plan specific to the qualifying condition must be created, maintained, and shared with all treating providers. At least one interactive communication with the patient or caregiver must occur per month. A minimum of 30 minutes of care activity must be logged per calendar month to bill the base PCM code. Circle Care's auto-timer tracks every qualifying minute across calls, care coordination, prescription reviews, and care plan updates in real time.
Medicare Coverage & Co-Pay Considerations
Medicare Part B covers 80% of the approved PCM amount, with patients responsible for a 20% co-pay — unless covered by Medigap, Medicare Advantage, or Medicaid. PCM can be billed concurrently with RPM in the same month, provided clinical time is tracked separately per program. PCM cannot be billed in the same month as CCM or TCM for the same patient. Circle Care flags all code conflicts automatically before any claim is submitted.
Everything You Need for PCM Success
Circle Care's PCM software handles the entire principal care management workflow — including real-time patient identification, condition-specific care plan creation, monthly care coordination, time tracking, and billing — so your team focuses on patients, not paperwork. No upfront investment. No new staff required.
Address Social Determinants of Health
Incorporate SDOH insights into every PCM care plan with guided assessments that uncover barriers to care, transportation challenges, food insecurity, and social isolation — enabling truly comprehensive, equitable disease management. For high-acuity single-condition patients, understanding the full clinical and social picture is what separates reactive care from effective care.
Streamline and Track Clinical Workflows
Assign tasks, monitor performance, and keep care teams aligned for greater efficiency and accountability. Circle Care's workflow engine routes condition-specific alerts, care plan review reminders, and overdue interaction flags to the right staff member automatically. No tasks fall through the cracks. No patient goes uncontacted.
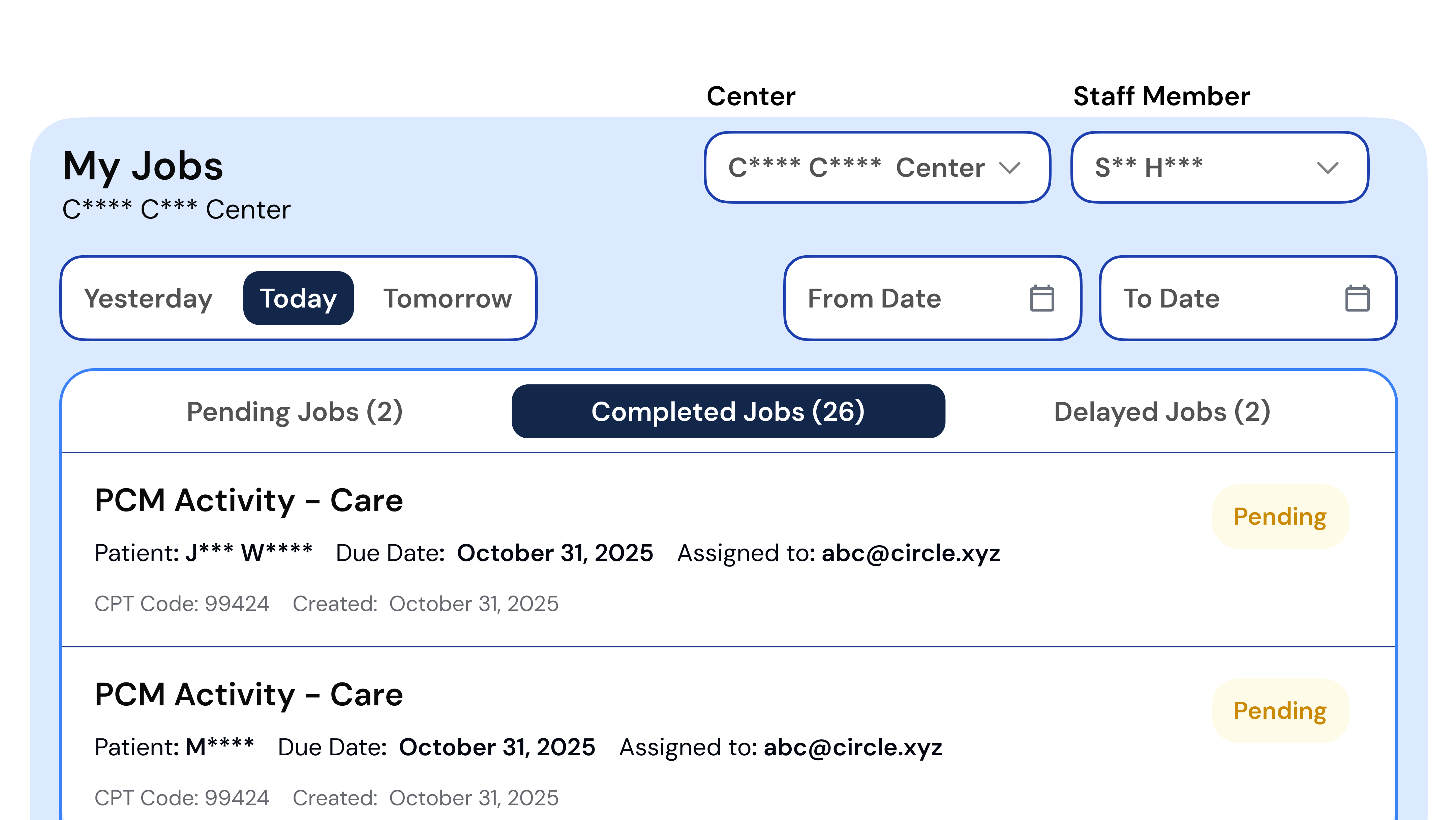
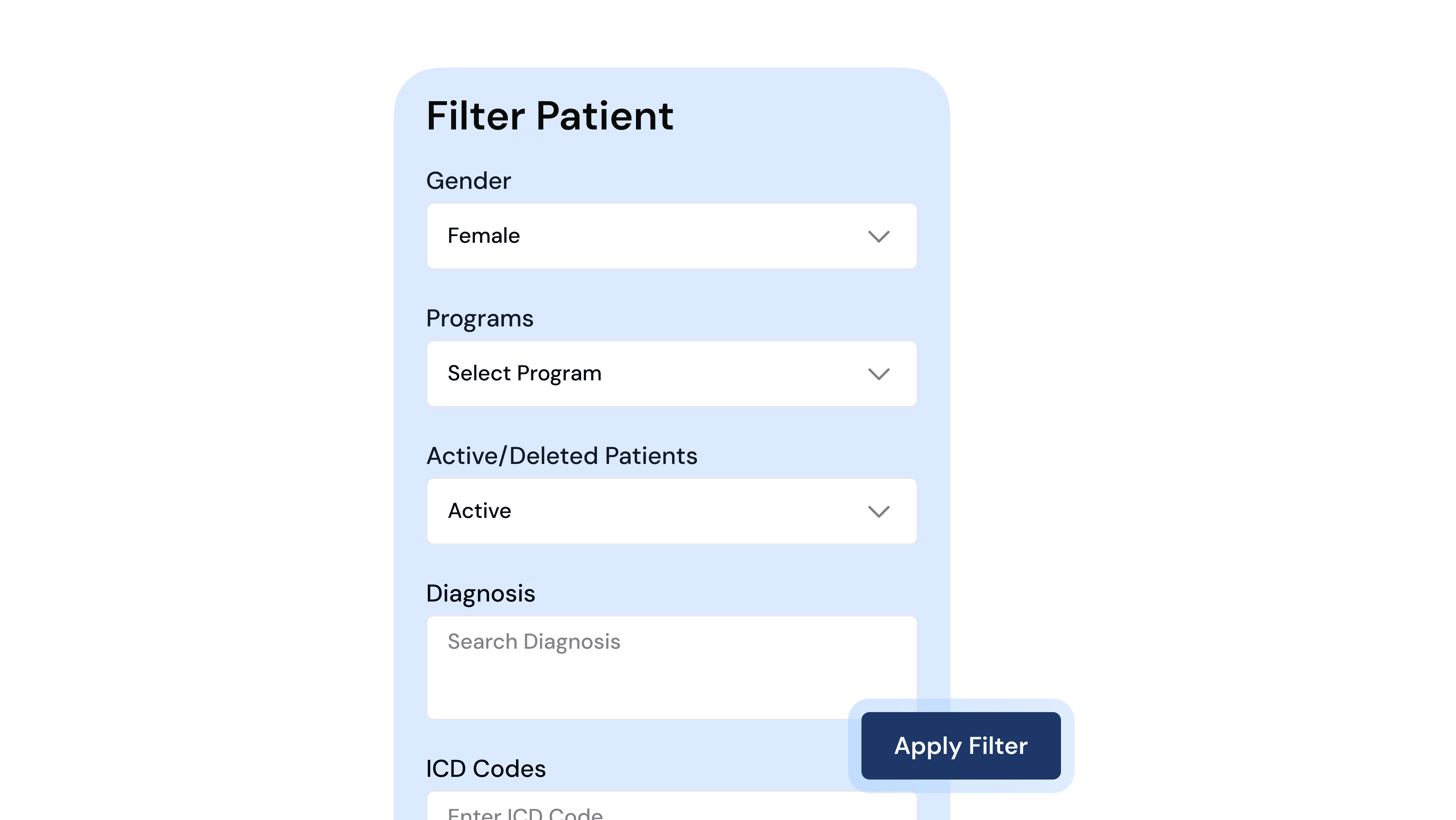
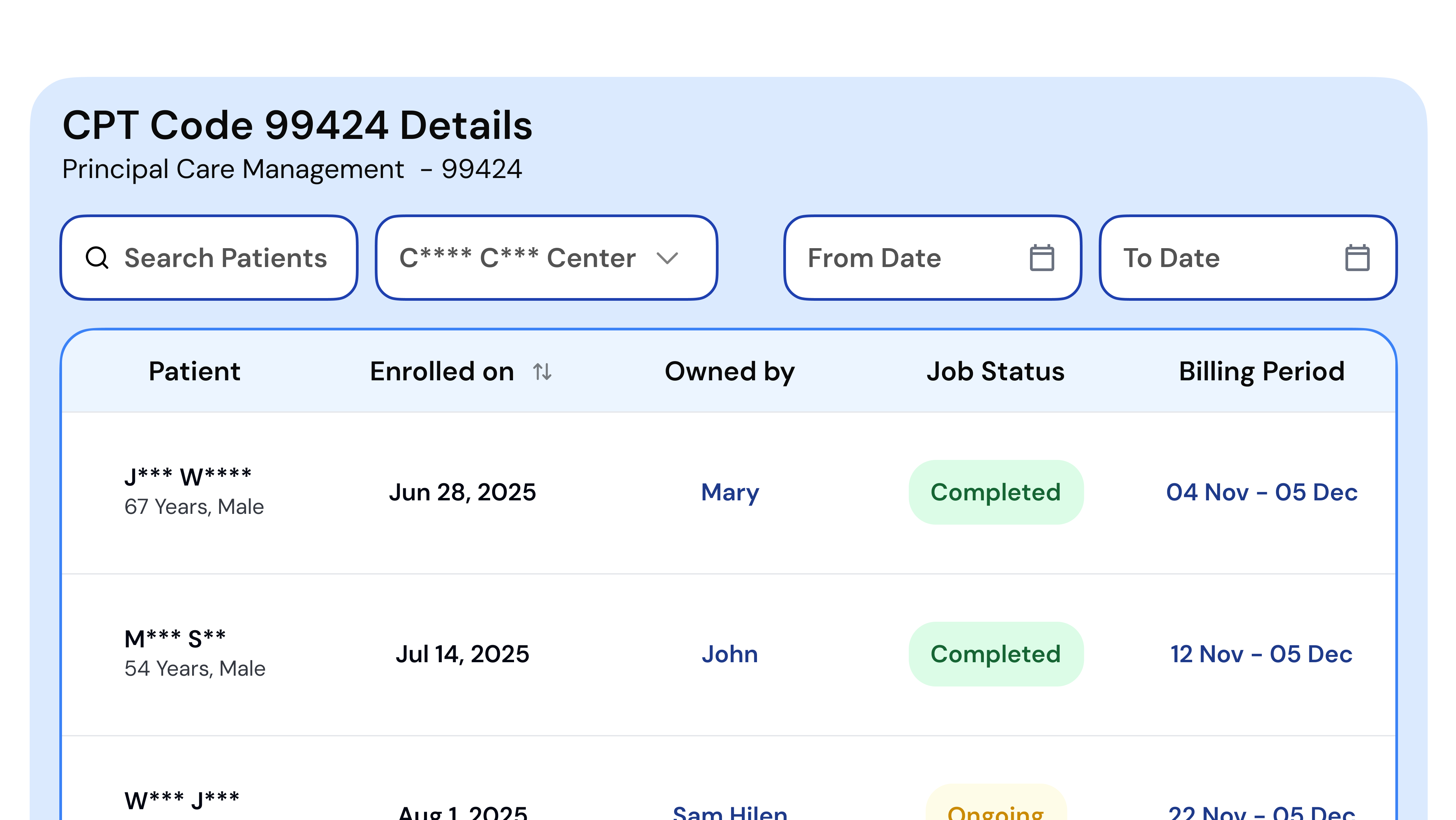
Manage Every PCM Patient Seamlessly
Use customizable filters and views to organize your entire PCM patient panel by care team, enrollment status, time logged, qualifying condition, and risk level — all in one place. Whether you're managing 50 patients or 500, Circle Care gives your team the visibility to prioritize, act, and bill accurately every single month.
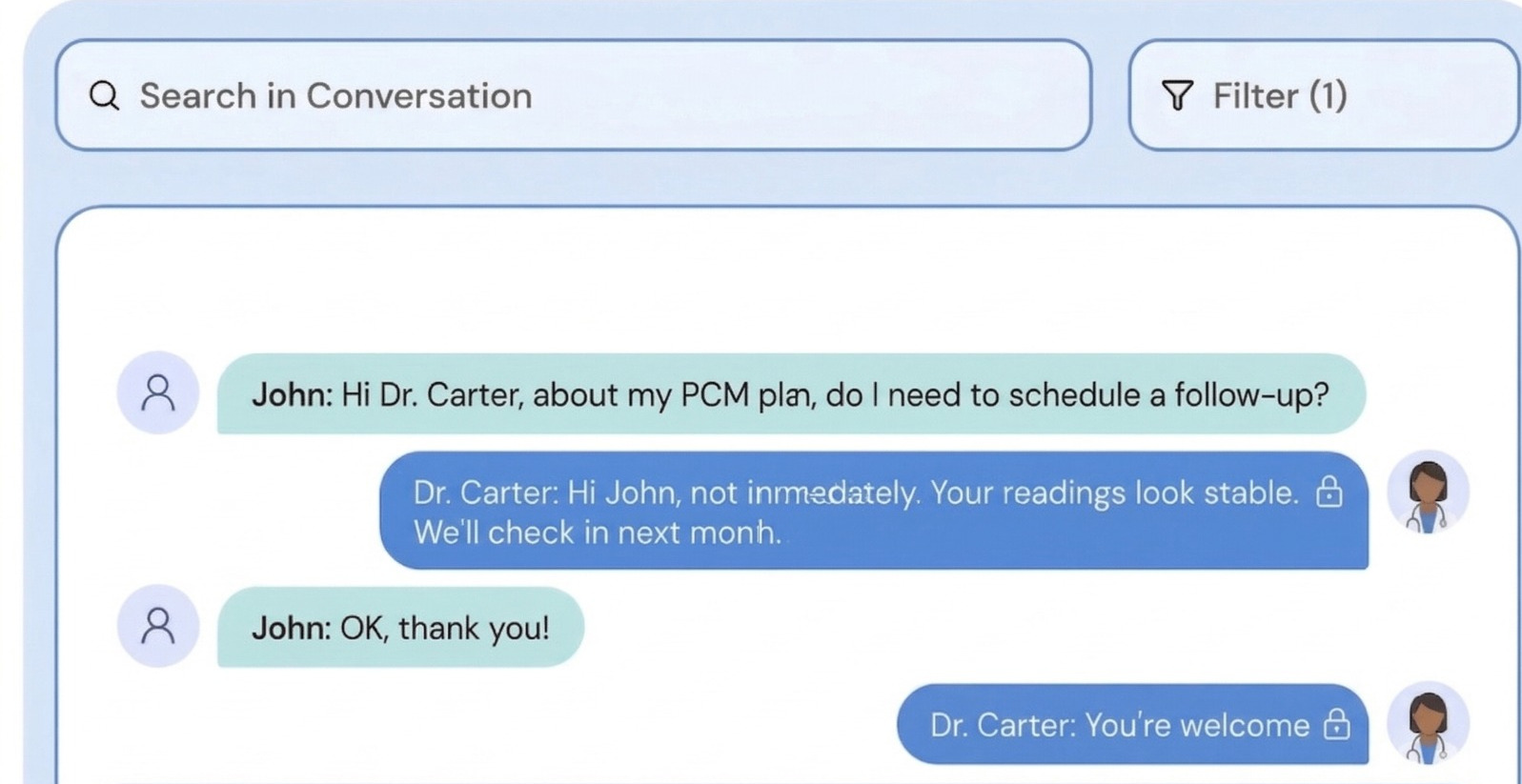
Engage Patients Through Secure Messaging
Enable HIPAA-compliant texting that keeps patients connected with their entire care team through one shared, secure conversation thread. For PCM patients managing a single high-acuity condition, consistent, accessible communication is not a nice-to-have — it is the intervention. Circle Care makes every touchpoint documented, trackable, and billable.
Automate and Track Billable Time
Circle Care's built-in timer activates automatically the moment a clinician opens a patient's PCM activity screen. Phone calls, care coordination, prescription reviews, referral management, and care plan updates are all logged in real time — with time totals tracked per program, per patient, per month. Compliance alerts notify care coordinators before the 30-minute billing threshold is missed.
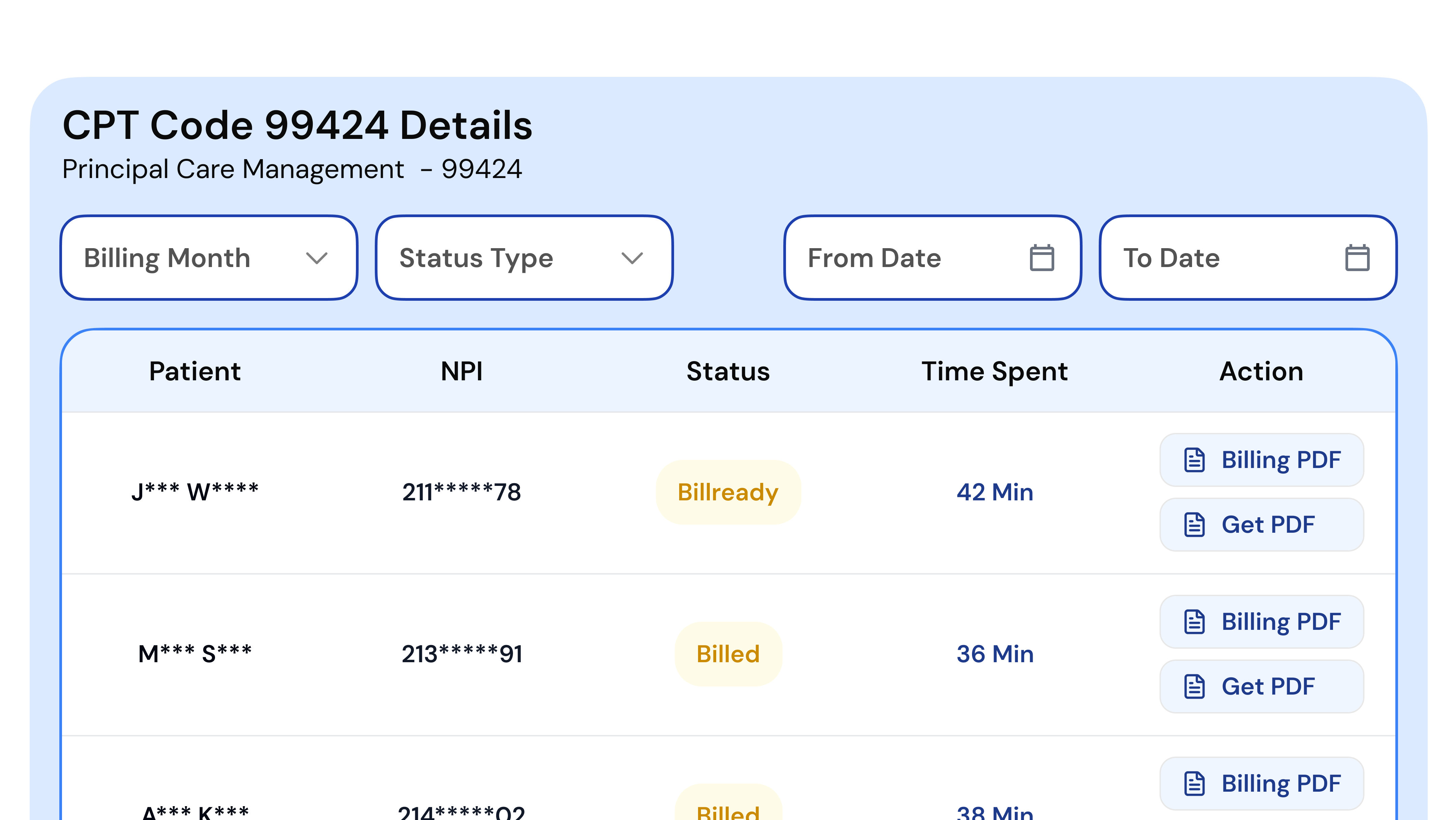
Simplify Your PCM Revenue Cycle
Track every patient interaction effortlessly and consolidate them into one ready-to-bill report. Circle Care maps all activity to the correct CPT code — 99424, 99425, 99426, or 99427 — based on who logged the time and how much was recorded. A billing readiness check runs before any claim goes out, flagging incomplete documentation, unmet thresholds, or code conflicts automatically. Review, approve, and submit — it's that seamless.
Billing & Codes
Auto-capture time & notes to bill accurately for CPT 99424, 99425, 99426 & 99427
EHR Integration
FHIR/HL7-compatible. Connects with major EHRs to eliminate double entry
Security & Compliance
HIPAA, SOC 2 Type II, ISO 27001. Enterprise-grade encryption and role-based access
The PCM Process with Circle Care: Step by Step
Circle Care structures PCM delivery across four CMS-aligned phases. Every milestone is tracked, documented, and flagged within the platform — so no episode falls through the cracks, and no revenue is left on the table. Most practices are fully operational within 2 weeks.
Identify & Enroll Eligible Medicare Patients
- AI-powered engine scans your panel for Medicare beneficiaries with single high-risk chronic conditions meeting CMS complexity criteria
- Eligible patients surfaced automatically; no manual chart reviews required
- Digital consent forms generated, sent, and tracked within Circle Care
- Enrollment logged and immediately audit-ready from day one
Create a Condition-Specific Care Plan
- Clinicians select from condition-specific PCM care plan templates built to CMS standards
- Key fields: diagnosis, medications, care goals, specialist contacts auto-populate from EHR data
- Care plan reviewed, finalised, and shared with all treating providers within the platform
- Template-to-finalised plan time: under 10 minutes per patient
Log Monthly Interactions & Track Clinical Time
- Built-in timer activates automatically during every patient PCM interaction
- Phone calls, care coordination, prescription reviews, and referral management all loggable in real time
- Live dashboard shows time logged per patient against the 30-minute billing threshold
- Compliance alerts notify coordinators when a patient approaches or misses the monthly minimum
Generate Compliant Billing Reports
- Month-end billing report generated automatically for every qualifying PCM patient
- Correct CPT code auto-assigned — 99424/99425 (physician) or 99426/99427 (clinical staff) — based on who logged time
- Full interaction logs, time documentation, and consent records attached to every report
- Report exported directly to your billing team or clearinghouse for fast, clean reimbursement
PCM CPT Codes & Principal Care Management Billing
Circle Care automatically applies the correct PCM CPT code — 99424, 99425, 99426, or 99427 — based on who is delivering the service and the total time documented per calendar month. No manual code selection. No missed reimbursement.
Note: Payment amounts are approximate national Medicare averages. Actual reimbursement varies by geographic location. Refer to cms.gov for the most current fee schedule.
- Service
- PCM — Physician / NPP, first 30 minutes
- Time required
- At least 30 minutes/month of physician or NPP-led care management
- Who bills it
- Physician or qualified non-physician practitioner
- Average Medicare payment
- ~$97
- Who qualifies
- Medicare patients with one serious, complex chronic condition — physician-directed
- Circle Care
- Auto-assigns code when physician time meets 30-minute threshold
- Service
- PCM — Physician / NPP, each additional 30 minutes
- Time required
- Each additional 30-minute increment beyond CPT 99424
- Billed with
- CPT 99424
- Average Medicare payment
- ~$71
- Who qualifies
- Same patient, same month — additional physician / NPP time documented
- Circle Care
- Auto-adds units as physician time thresholds are met
- Service
- PCM — Clinical staff, first 30 minutes
- Time required
- At least 30 minutes/month of supervised clinical staff care management
- Who bills it
- Clinical staff under the general supervision of the billing physician or NPP
- Average Medicare payment
- ~$74
- Who qualifies
- Medicare patients with one serious, complex chronic condition — staff-delivered
- Circle Care
- Auto-assigns code based on staff time logged, separate from physician time
- Service
- PCM — Clinical staff, each additional 30 minutes
- Time required
- Each additional 30-minute block beyond CPT 99426
- Billed with
- CPT 99426
- Average Medicare payment
- ~$57
- Who qualifies
- Same patient, same month — additional supervised clinical staff time documented
- Circle Care
- Auto-adds units as staff time thresholds are met
Billing Best Practices
PCM claims are submitted monthly, with the service period covering the calendar month. PCM cannot be billed in the same month as CCM, APCM, or TCM for the same patient. PCM and RPM can be billed concurrently, provided clinical time for each service is tracked and documented separately. Circle Care's billing prep module runs a readiness check before any claim goes out — flagging incomplete documentation, unmet time thresholds, or code conflicts automatically.
Common Billing Errors Circle Care Prevents
PCM Documentation Requirements — What a Compliant Care Plan Includes
Complete, accurate documentation is the foundation of a defensible PCM claim. Circle Care's condition-specific care plan templates pre-populate required fields from your connected EHR — reducing manual entry, minimising errors, and ensuring every enrolled patient is audit-ready from day one.
Required Documentation Checklist
- Patient consent record — date, method, and annual renewal status documented
- Qualifying condition — diagnosis, severity, and complexity justification documented
- Condition-specific care plan — goals, medications, care team contacts, and specialist coordination
- Monthly interaction log — date, time, method, and summary of every patient contact
- Time documentation — physician time and clinical staff time tracked separately per CPT code
- Medication reconciliation record — current medications, dosages, and adherence notes
- Care plan revision history — version-controlled updates with timestamps
Documentation Example Breakdown
“Written consent obtained 04/10/2025 at 11:00 AM. Patient informed of PCM program scope, cost-sharing responsibility, right to opt out, and that only one provider may bill PCM per calendar month. Consent logged and timestamped in Circle Care platform.”
“Principal condition: Systolic Heart Failure (I50.20), NYHA Class III. Condition expected to last > 3 months. Risk of hospitalisation and functional decline documented. Care goals: reduce hospitalisation frequency, maintain weight within 2 lbs of baseline, optimise diuretic therapy. Care plan created 04/10/2025, shared with cardiologist and home health team.”
“Phone contact 05/01/2025 at 3:30 PM by RN Care Manager. Patient reported weight gain of 3 lbs over 3 days; physician notified, diuretic dose adjusted. Time logged: 34 minutes (clinical staff). CPT 99426 threshold met. Logged in Circle Care platform.”
High-Risk Chronic Conditions We Support Under PCM
Circle Care's PCM platform includes condition-specific care plan templates, clinical workflows, and alert configurations for the high-acuity conditions most commonly managed under principal care management.
Heart Failure & Cardiovascular Disease
Heart failure is one of the most common PCM-qualifying conditions. Circle Care supports daily weight monitoring via connected smart scales, fluid management tracking, medication adherence alerts, and cardiology-specific care plan templates. Integration with RPM allows real-time weight and blood pressure data to feed directly into the PCM dashboard.
Learn MoreCOPD & Respiratory Conditions
Advanced COPD and severe asthma patients require consistent lung function monitoring and exacerbation prevention. Circle Care's PCM module includes oxygen saturation tracking, inhaler adherence logging, and pulmonology-specific escalation pathways — keeping high-risk respiratory patients out of the emergency room.
Learn MoreDiabetes with Complications
Diabetic patients with nephropathy, neuropathy, or retinopathy require intensive, condition-focused management beyond standard CCM. Circle Care integrates glucometer and CGM data, tracks HbA1c trajectory, monitors foot care compliance, and coordinates across endocrinology, nephrology, and ophthalmology.
Learn MoreCancer & Oncology
Active oncology patients face complex, rapidly changing clinical needs. Circle Care's PCM module supports symptom burden tracking, weight and temperature monitoring, treatment toxicity alerts, and seamless communication between oncologists, primary care, and palliative care teams.
Learn MoreDementia & Neurological Conditions
Patients with Parkinson's, MS, ALS, or moderate-to-severe dementia require coordinated, condition-specific management. Circle Care supports cognitive assessment completion, caregiver communication tools, and neurology coordination notes — all within a single PCM care plan and a full audit trail.
Learn MoreChronic Kidney Disease (Stage 4–5)
CKD at advanced stages requires intensive monitoring to slow progression and manage complications. Circle Care's PCM templates cover eGFR and creatinine tracking, dietary and fluid management guidance, medication reconciliation, and nephrologist coordination — all documented and billable within the PCM framework.
Learn MorePair PCM with Other Value-Based Care Programs
PCM is one of six CMS care programs on Circle Care. Combine it with RPM, CCM, or BHI to build a complete, revenue-generating care ecosystem — all on one platform, one team.
Chronic Care Management
Continuous, coordinated support for patients with 2+ chronic conditions. Improve outcomes between visits.
Learn MoreRemote Patient Monitoring
Real-time vitals tracking to prevent complications and reduce hospital readmissions between appointments.
Learn MoreTransitional Care Management
Coordinated post-discharge support to reduce readmissions during the critical 30-day transition window.
Learn MoreBehavioral Health Integration
Integrate behavioral health into everyday primary care to address the whole patient, not just the condition.
Learn MoreAdvanced Primary Care Management
Population-based care management for practices delivering advanced, comprehensive primary care.
Learn MoreCare Management Services
Our team of licensed RNs and medical assistants works as an extension of your practice. No new hires needed.
Learn More“Circle Care has transformed the way we deliver care, helping us spot gaps early, stay connected with patients between visits, and act faster when it matters most. Their team feels like an extension of ours, combining smart technology with real, human support.”
Principal Care Management — Questions Answered
PCM is a Medicare-reimbursed program providing monthly, intensive care coordination for patients with one serious, complex chronic condition that carries a risk of acute exacerbation, hospitalisation, or functional decline. It was introduced by CMS effective January 1, 2023, and fills the gap for patients whose single dominant condition requires more focused management than CCM provides.
CCM covers patients with two or more chronic conditions and requires 20 minutes of monthly clinical staff time. PCM covers patients with one high-risk condition, requires 30 minutes of care activity per month, and carries higher per-code reimbursement. They cannot be billed for the same patient in the same calendar month. Circle Care manages both programs in a single platform with separate time tracking and billing cycles for each.
CPT 99424 covers physician or NPP-led PCM for the first 30 minutes per month (~$97). CPT 99425 covers each additional 30 minutes of physician time (~$71). CPT 99426 covers the first 30 minutes of supervised clinical staff time (~$74). CPT 99427 covers each additional 30 minutes of clinical staff time (~$57). Circle Care auto-assigns the correct code based on who logged time and how much was recorded.
Yes. PCM and Remote Patient Monitoring can be billed concurrently for the same patient in the same month, provided the clinical time for each service is tracked and documented separately. Circle Care automates this tracking, with no double-counting and full compliance.
Cardiology, pulmonology, endocrinology, oncology, and neurology benefit most, given the high-acuity, single-condition patient populations they manage. PCM is also well-suited for primary care practices managing severe COPD, uncontrolled diabetes with complications, or advanced heart failure patients.
CMS does not publish a fixed list, but qualifying conditions typically carry a documented risk of acute exacerbation, hospitalisation, or significant functional decline. Common examples include heart failure, advanced COPD, diabetes with complications, cancer, CKD Stage 4–5, dementia, and neurological conditions such as Parkinson's or MS. Severity and complexity are the deciding factors — not the diagnosis name alone.
Yes. A patient may be in PCM one month and CCM the next based on clinical need and provider judgement — but only one program may be billed per calendar month. The transition must be documented in the medical record. Circle Care flags the change and ensures no concurrent billing conflict occurs.
You will need: written patient consent, the condition-specific care plan with revision history, monthly interaction logs with timestamps and staff identifiers, time documentation separated by CPT code, and evidence of at least one interactive patient communication per month. Circle Care stores and exports all of this automatically — ready in one click.
PCM is billed monthly. The correct CPT code is determined by who delivers the service (physician/NPP vs. supervised clinical staff) and the total time documented. Circle Care auto-assigns codes, runs a billing readiness check, and generates a submission-ready report at month-end with full interaction logs attached.
Most practices are live and billing within two weeks of onboarding. Circle Care handles EHR integration, care plan template configuration, staff training, and patient enrollment — all managed by Circle Care's implementation team at no additional cost.
Latest Insights on Principal Care Management
Operationalizing PCM Without Hiring New Staff
How practices can launch a fully compliant PCM program using existing clinical resources — covering patient identification, care plan workflows, and billing setup from day one.
CPT Code 99424 for Billing Principal Care Management
A practical breakdown of CPT 99424 — who qualifies, what documentation is required, how it differs from 99426, and how to avoid the most common PCM billing errors.
What Is Principal Care Management & How It Works
A complete guide to PCM — CMS requirements, eligible conditions, the difference from CCM, CPT codes, and how Circle Care makes compliance effortless.
Ready to Start Your Principal Care Management Program?
Let's design a PCM program that delivers intensive, focused care for your highest-risk patients and grows sustainable practice revenue with zero upfront cost and no new staff needed.
Revenue snapshot: 100 PCM patients at CPT 99424 = ~$9,700/month. Add RPM, and the number climbs further.