Keep High-Risk Patients Out of the Hospital — Seamless Post-Discharge Support
Circle Care's AI-powered TCM platform tracks every discharge, coordinates every transition, and keeps your team CMS-compliant — protecting patient outcomes and practice revenue from day one.
TCM Compliance at a Glance
- Real-time ADT alerts on every discharge
- Interactive contact within 2 business days tracked
- Medication reconciliation recorded and reviewed
- Discharge summary shared across the care team
- Face-to-face visit within 7 or 14 days automated reminders
- CPT 99495 or 99496 auto-applied
- Full audit trail for every TCM episode
What Is Transitional Care Management?
Transitional Care Management (TCM) is a structured, CMS-defined care model that provides coordinated support to high-risk patients during the critical 30-day window following discharge from a hospital, observation stay, or skilled nursing facility. It exists to close the gap between inpatient and outpatient care — the period when patients are most vulnerable to complications and readmission.
TCM meaning in practice: it's proactive, not reactive. Rather than waiting for a patient to deteriorate or call in, your team initiates contact, reconciles medications, coordinates follow-up care, and ensures a safe, documented return to community-based care. Circle Care makes that entire process automatic — from discharge alert to billing submission.
Who Qualifies for TCM?
- Discharged from inpatient acute care hospitals
- Discharged from observation status stays
- Discharged from skilled nursing facilities (SNF)
- Discharged from long-term care hospitals (LTCH)
- Discharged from inpatient rehab facilities (IRF)
- Within the 30-day post-discharge CMS window
- Returning to a community setting
TCM vs. Standard Follow-Up Care
| Area | Traditional Follow-Up | TCM with Circle Care |
|---|---|---|
| First contact | Patient-initiated | Within 2 business days — automated alert |
| Medication review | At appointment only | Reconciled and recorded immediately |
| Care coordination | Ad hoc | Structured, documented, trackable |
| Billing | Standard E&M codes | CPT 99495 / 99496 auto-applied |
| Readmission risk | Unmanaged | Actively reduced with real-time monitoring |
| Compliance tracking | Manual or none | AI-powered, full audit trail |
CMS Transitional Care Management Requirements
CMS defines TCM as a set of coordinated services delivered to Medicare beneficiaries during the 30 days following discharge — designed to reduce avoidable readmissions. Two CPT codes, 99495 and 99496, govern reimbursement based on medical decision complexity and face-to-face visit timing.
Circle Care's platform is built around these requirements. Every milestone contact, coordination, and visit is tracked, time-stamped, and audit-ready before a claim is ever submitted.
Interactive Contact Within 2 Business Days
Within 2 business days of discharge, your care team must make an interactive phone, telehealth, or in-person contact with the patient or caregiver. Voicemail does not qualify. Circle Care's real-time ADT alerts prompt your care team the moment a discharge is detected, so the 2-day window is never missed.
Non-Face-to-Face Services
Ongoing care coordination between the first contact and the face-to-face visit. Includes medication reconciliation, care plan documentation, referral management, and patient and caregiver education — all logged within Circle Care and tied to the patient's TCM episode.
Face-to-Face Visit
Required within 7 days of discharge for high complexity (CPT 99496) or 14 days for moderate complexity (CPT 99495). This visit triggers billing. Circle Care auto-assigns the correct CPT code based on documented complexity and sends automated reminders to reduce no-shows.
Everything You Need for TCM Success
Circle Care's TCM software handles the entire post-discharge workflow — including real-time discharge detection, care coordination, documentation, and billing — so your team focuses on patients, not paperwork. No upfront investment. No new staff required.
Connect Every Data Point
Seamlessly integrate EHRs, data exchanges, remote monitoring tools, and mobile apps to create a complete, connected view of every patient.
Stay Ahead of Upcoming Discharges
Track expected discharge dates and locations to plan timely, coordinated follow-up care before patients ever leave the facility.
Keep Stakeholders Informed at Every Step
Share detailed discharge summaries across your care team to track each stage of care, support TCM billing, and secure timely reimbursement.
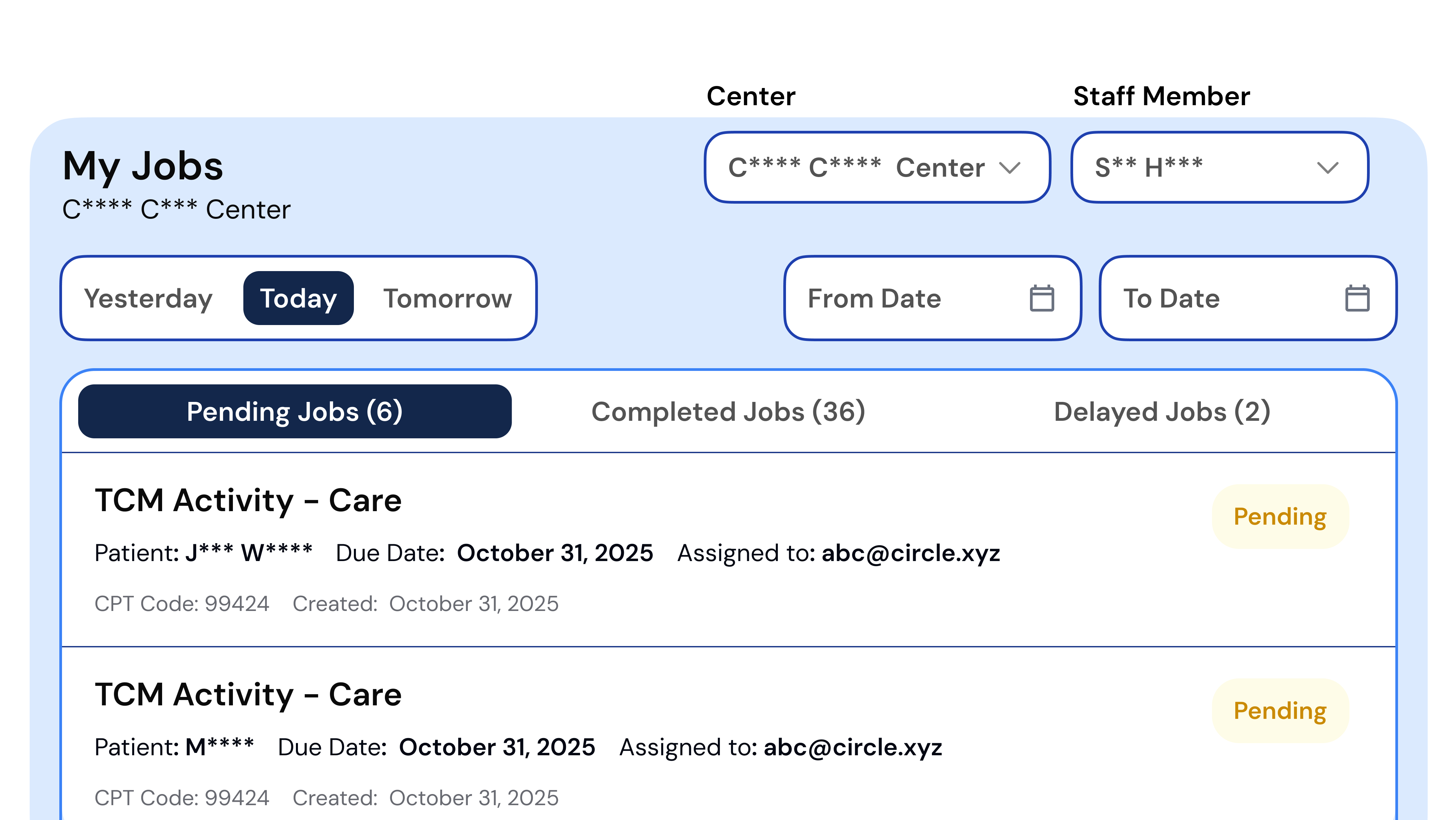
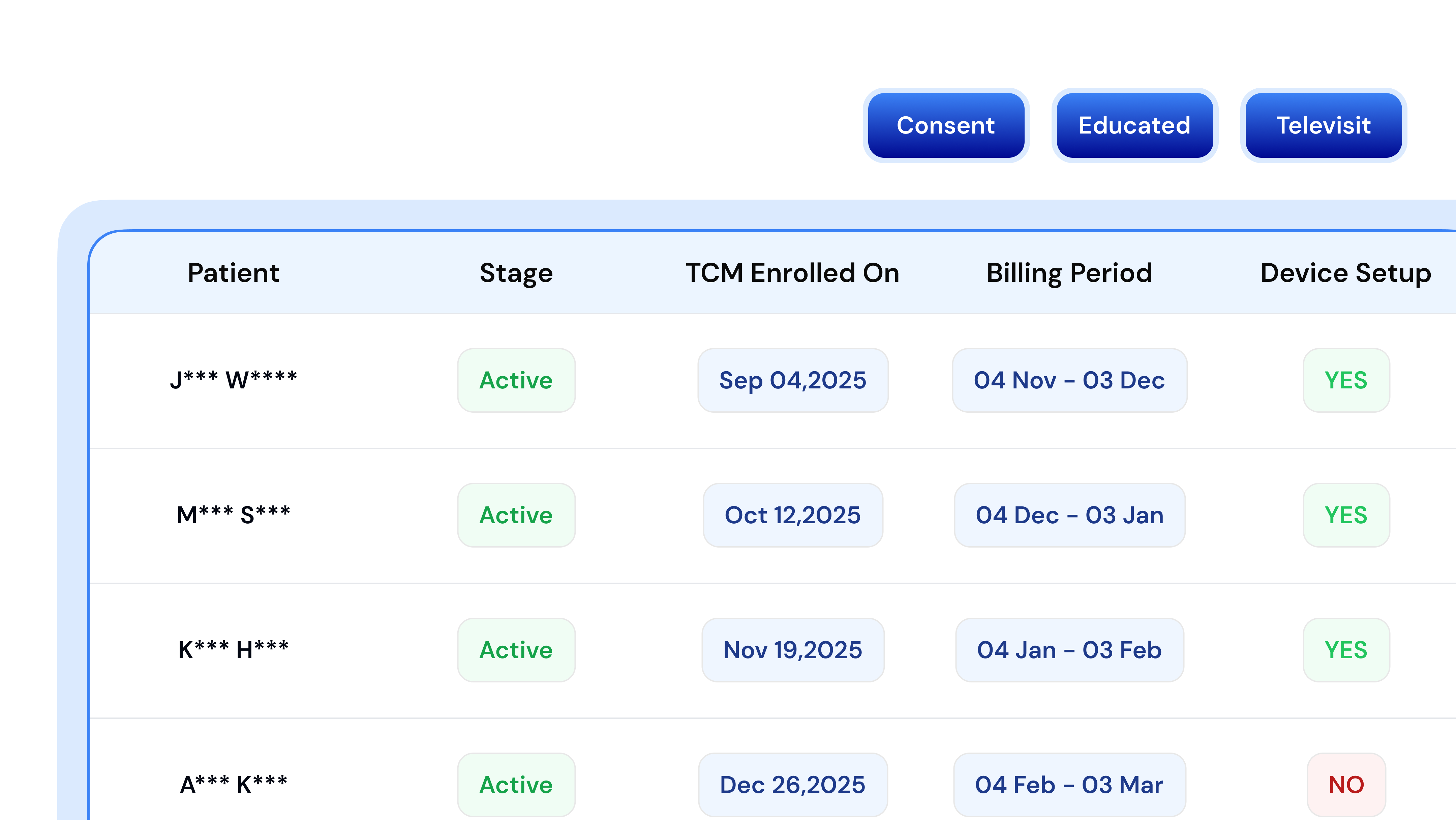
Track Every Patient Transition
Record patient interactions, streamline workflows, and keep your entire care team connected and informed throughout the 30-day episode.
Support Medication Adherence When It Matters Most
Record and review medication details to help patients stay informed and on track with their post-discharge treatment plan.
Simplify Billing and Compliance
Automatically apply TCM CPT codes — 99495 and 99496 — for faster, more accurate reimbursement with full audit trails on every claim.
Billing & Codes
Auto-capture time & notes to bill accurately for CPT 99495 & 99496
EHR Integration
FHIR/HL7-compatible. Connects with major EHRs to eliminate double entry
Security & Compliance
HIPAA, SOC 2 Type II, ISO 27001. Enterprise-grade encryption and role-based access
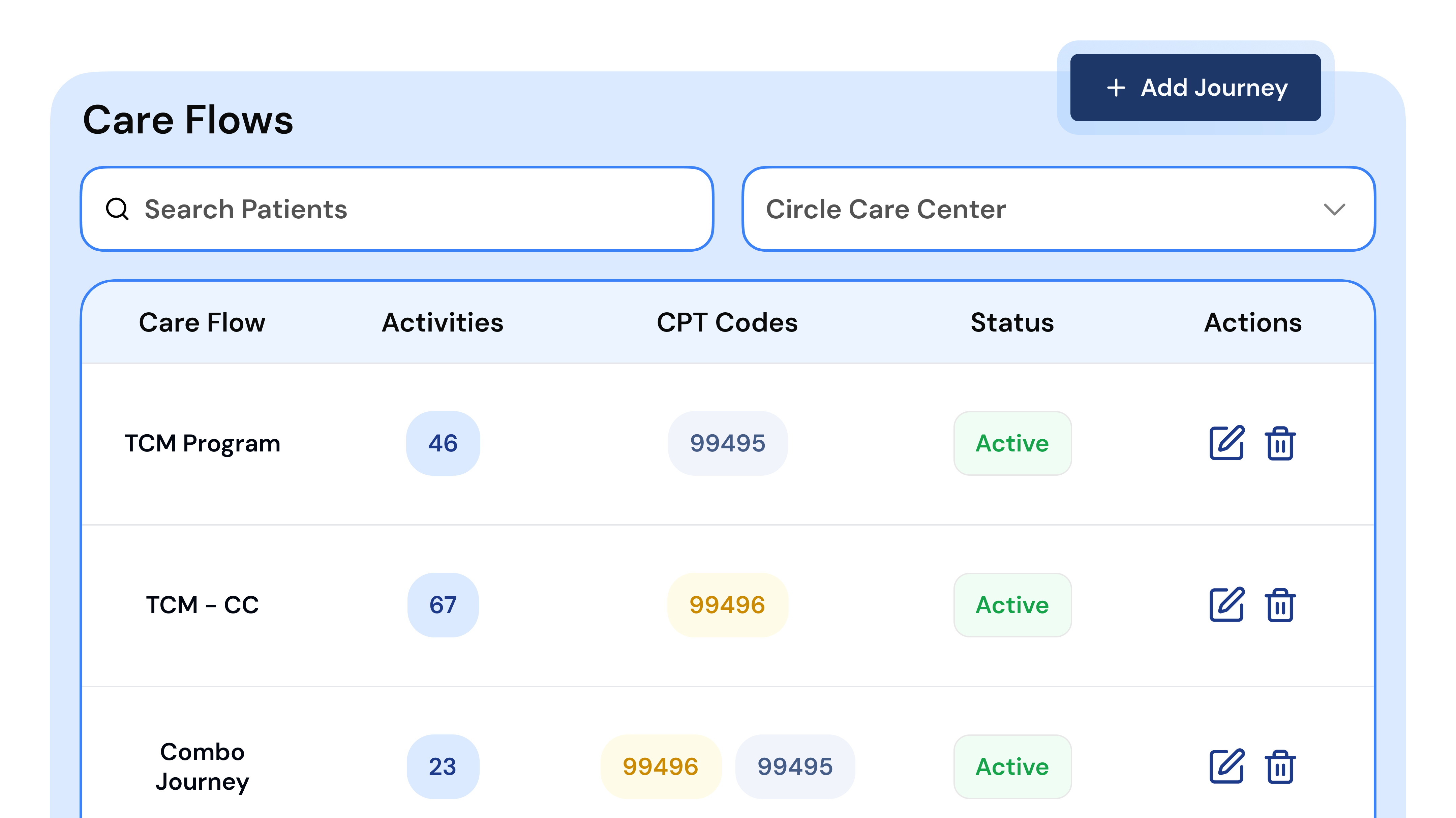
The TCM Process with Circle Care: Step by Step
Circle Care structures TCM delivery across three CMS-aligned phases. Every milestone is tracked, documented, and flagged within the platform — so no episode falls through the cracks and no revenue is left on the table.
Interactive Contact Within 2 Business Days of Discharge
- Real-time ADT alert triggers care team notification on discharge
- Phone or telehealth contact made with patient or caregiver
- Condition, medication concerns, and follow-up needs assessed
- Date, time, method, and summary are auto-documented in Circle Care
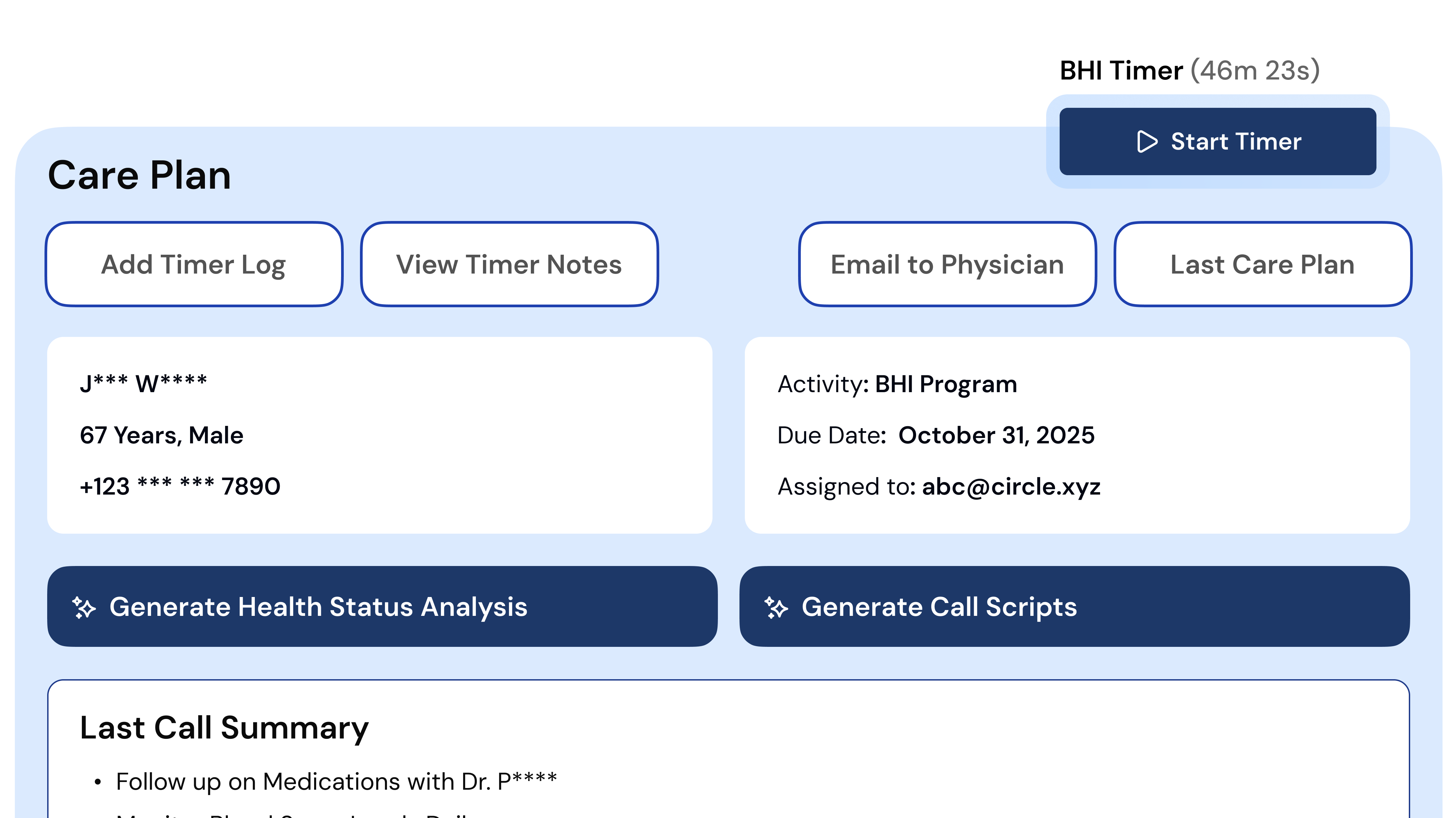
Non-Face-to-Face Services Ongoing Between Contact and Visit
- Medication reconciliation completed and discrepancies flagged
- Care plan developed, documented, and shared across the care team
- Specialist referrals coordinated and tracked in the platform
- Patient and caregiver education delivered and logged
Face-to-Face Visit Within 7 Days (99496) or 14 Days (99495)
- Automated patient reminders sent to reduce no-shows
- Physician or qualified provider visit completed
- Medical decision complexity pulled from documented visit notes
- CPT 99495 or 99496 auto-applied; billing readiness check run before submission
CPT Codes for Transitional Care Management
Circle Care automatically applies the correct TCM CPT code — 99495 or 99496 — based on documented medical decision complexity and face-to-face visit timing. No manual code selection. No missed reimbursement.
- Complexity
- Moderate Medical Decision-Making
- Face-to-face visit
- Within 14 days of discharge
- Interactive contact
- Within 2 business days
- Average Medicare payment
- ~$176
- Who qualifies
- Post-discharge patients with manageable, moderate-complexity conditions
- Circle Care
- Auto-assigns code when all documentation criteria are met
- Complexity
- High Medical Decision-Making
- Face-to-face visit
- Within 7 days of discharge
- Interactive contact
- Within 2 business days
- Average Medicare payment
- ~$236
- Who qualifies
- Patients with high-risk diagnoses, complex polypharmacy, or recent ICU stay
- Circle Care
- Auto-assigns code; complexity justification pulled from visit documentation
Billing Best Practices
TCM claims are submitted after the face-to-face visit is completed, using the date of discharge as the service start date. Circle Care's billing prep module runs a readiness check before any claim goes out, flagging incomplete documentation, missed milestones, or code conflicts automatically.
Common Billing Errors Circle Care Prevents
TCM Documentation Requirements & Worksheet
Complete, accurate documentation is the foundation of a defensible TCM claim. Circle Care's built-in templates pre-populate required fields from your connected EHR — reducing manual entry, minimising errors, and ensuring every episode is audit-ready.
Required Documentation Checklist
- Interactive contact date & method — date and time recorded automatically
- Diagnosis & discharge summary — facility, date, primary and secondary diagnoses
- Medication reconciliation record — pre vs. post-discharge comparison, discrepancies flagged
- Care plan & follow-up schedule — referrals, education, and appointments logged
- Face-to-face visit notes — complexity determination and provider attestation
Documentation Example Breakdown
“Phone contact made 04/28/2025 at 10:15 AM by RN. Patient reported dizziness post-discharge; medication was reviewed, and the physician was notified. Logged in Circle Care platform.”
“Pre-discharge: Metoprolol 25mg. Post-discharge: Metoprolol 50mg (dose adjusted). Patient counselled. Discrepancy flagged and resolved in Circle Care.”
“Office visit 05/05/2025. High complexity MDM. Patient stable. Care plan reviewed. CPT 99496 auto-applied by Circle Care platform.”
TCM Questions — Answered
TCM is a structured CMS care model providing coordinated support to high-risk patients for 30 days after discharge from inpatient, observation, or skilled nursing settings. It includes proactive outreach, medication reconciliation, care coordination, and a follow-up face-to-face visit — all designed to prevent readmission. Circle Care automates the entire process.
CMS requires: (1) interactive contact within 2 business days; (2) non-face-to-face services including medication reconciliation and care coordination; and (3) a face-to-face visit within 7 days (high complexity) or 14 days (moderate complexity), all within the 30-day post-discharge period. Circle Care tracks every milestone in real time.
CPT 99495 covers moderate medical decision complexity with a 14-day face-to-face window (avg. payment ~$176). CPT 99496 covers high complexity with a 7-day window (avg. payment ~$236). Circle Care auto-assigns the correct code based on documented complexity.
TCM is billed after the face-to-face visit is completed, using the discharge date as the service start. Circle Care runs automated readiness checks — verifying all three phases are complete and no code conflicts exist — before any claim is submitted.
Required: interactive contact date and method, discharge diagnosis and summary, medication reconciliation record, care plan with follow-up schedule, and face-to-face visit notes with complexity determination. Circle Care templates and EHR integration pre-populate and audit-trail all fields.
Circle Care automates discharge detection (ADT alerts), contact tracking, care coordination, medication reconciliation, documentation, CPT code assignment, and billing readiness checks. HIPAA, SOC 2 Type II, and ISO 27001 certified. Zero upfront cost. No new staff required.
Pair TCM with Other Value-Based Care Programs
TCM is one of six CMS care programs on Circle Care. Combine it with CCM, RPM, or BHI to build a complete, revenue-generating care ecosystem — all on one platform, one team.
Chronic Care Management
Continuous, coordinated support for patients with 2+ chronic conditions. Improve outcomes between visits.
Learn MoreRemote Patient Monitoring
Real-time vitals tracking to prevent complications and reduce hospital readmissions between appointments.
Learn MoreBehavioral Health Integration
Integrate behavioral health into everyday primary care to address the whole patient, not just the condition.
Learn MorePrincipal Care Management
Focused management for patients with a single, high-risk chronic condition requiring intensive coordination.
Learn MoreAdvanced Primary Care Management
Population-based care management for practices delivering advanced, comprehensive primary care.
Learn MoreCare Management Services
Our team of licensed RNs and medical assistants works as an extension of your practice. No new hires needed.
Learn More“Circle Care has transformed the way we deliver care — helping us spot gaps early, stay connected with patients between visits, and act faster when it matters most. Their team feels like an extension of ours, combining smart technology with real, human support.”
Latest Insights on Transitional Care
Low-Friction Transition of Care Management for Health Systems
How health systems can streamline care transitions with ADT alerts, structured workflows, TCM billing, and outsourced support to reduce readmissions at scale.
CPT Code 99495 for Billing Transitional Care Management
A practical breakdown of CPT 99495 — who qualifies, what documentation is required, and how to avoid the most common billing errors.
What Is Transitional Care Management & How It Works
A complete guide to TCM meaning, CMS requirements, the three-phase process, and how Circle Care makes compliance manageable.
Ready to Strengthen Your Transitional Care Program?
Let's design a TCM program that keeps your patients out of the hospital and grows sustainable practice revenue — with zero upfront cost and no new staff needed.